

Today, I am speaking with the one, the only Al Lewis, and we’re gonna talk about how 6% of a lot of plan sponsors’ total spend is now going to ER/ED (emergency room/emergency department) visits. That’s a lot of spend.
For a full transcript of this episode, click here.
If you enjoy this podcast, be sure to subscribe to the free weekly newsletter to be a member of the Relentless Tribe.
Al digs into this, so I’m just going to gloss over it all and make my own points or two along the way, I am sure here, as the intro.
But the reason why ERs are costing so much these days is, number one, because ER volume nationwide is, in fact, trending up (ie, more patients are going to the ER). We had a pandemic in the mix, so it’s a little sketchy to track, but yeah, the volume of ER visits per capita seems to be increasing—and it’s increasing faster than the population.
And number two reason, at the same time, the average cost per visit is going up. So there’s a bunch of things that I’m gonna say today where if you want to dig in on them, check out the stats here. But volume is going up. Also, the price per visit is going up. Let’s linger a little here on the price per visit part of the equation.
The average cost per visit went up 15% in 2023, which is something that Al brings up in the conversation that follows in a little bit greater depth. Now, in the context of ER visits becoming more expensive, here’s a common question that gets posed.
Is this increased cost because (A) ER visits are being upcoded, or (B) are patients showing up in the ER actually sicker?
Now I do realize that is an either-or, and most of us listening today and also many who pose this question and certainly Al Lewis are fully aware that there is other stuff going on. But let’s just keep it simple with this either-or binary before we make it more complicated. So, are ER visits being upcoded, or are patients sicker?
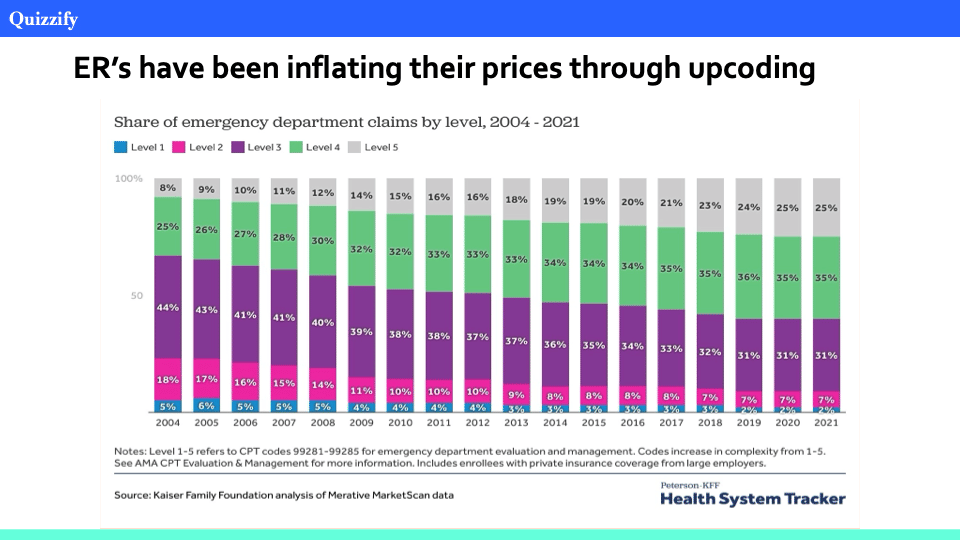
There is a right answer to that question, by the way, although not everyone wants to hear it. So, let us begin with it is a verifiable fact that visits are being coded at higher acuities than in the past. And the higher the coding acuity, the more the ER visit is going to cost, just to state the obvious. That’s why there is a financial reason to upcode—because the higher codes have higher associated prices.
Brian Cotter on LinkedIn the other day cites an ER coding analysis, and Al Lewis sent me a KFF (Kaiser Family Foundation) slide basically showing the same thing. ER visits are being coded at higher acuity. But it all boils down to, as Brian put it in that LinkedIn post, a notable shift toward higher-intensity coding in physician billing.
So, codes are upped, but are the patients actually sicker, thus warranting the higher acuity codes? Again, is there an increase in actual patient acuity, or is it just a change in coding practices jacking the codes up to higher severity levels?
Let me leave you on the edge of your seat just a moment here while I tick through some of the proposed answers to this question whether patients are sicker, thus requiring higher levels of coding acuity. You will certainly get some folks, very, very definitely, with three underlines, talking about their premise that urgent care has siphoned off most of the low-acuity cases that were going to ERs in the past, which has left hospital ERs with higher-acuity cases.
So, there is certainly a crew who is firmly in the “yes, patients are actually sicker” camp. Is this actually true, as per the data, that sicker patients are showing up in the ER? Well … no, not that I could find. And if you have stats showing otherwise, certainly send them over.
I did, however, find a KFF Health News examination of physician upcoding, which found that minor procedures such as removing a splinter or treating a wart are increasingly being billed as surgery, costing hundreds of dollars. Then I asked Al Lewis whether there’s evidence of higher-acuity patients showing up because urgent cares are dealing with the easy stuff. And he wrote me back with references.
He said if visits were actually higher acuity, then you would see a commensurate increase in hospital admissions aligned with that acuity. If, on the other hand, upcoding was the cause of more level 4 and level 5 visits, like the KFF Health News examination revealed, then you would see a reduction in admissions to the hospital from those codes.
And that is apparently what happened quite dramatically in California, where it was actually studied. Check out the study, showing way lower hospital admissions from the way higher acuity codes. So, yeah … upcoding.
And number two reason ERs are costing so much these days: Also, again, ER volume nationwide is in fact trending up.
And a third issue that Al talks about for ER total spend becoming more expensive is just, it’s really, really difficult for plan sponsors to negotiate for ER services. They are emergencies. Nobody can navigate.
A fourth factor that Al Lewis talks about in the show that follows is some shifts in what has been going on for in-network patients since the No Surprises Act. And again, we take that up in the conversation that follows.
So, four factors underpinning the rise in emergency room spend, but there’s kind of an underlying dynamic here that I want to bring up—and it’s kind of interwoven through a lot of the conversation.
I want to quote John Lee, MD, who is, in fact, an emergency room physician. When I gave him kind of the run of show on this episode, Dr. John Lee said to me:
“Here’s an anecdote from today. I just saw a young patient with abdominal pain. She has had symptoms on and off for months and has had little progress getting any attention from her primary physician.
“I could theoretically do some screening and labs and then have her scheduled for an office recheck tomorrow. But I had zero faith that she will actually get in to the office in follow-up. Also, even if she did and something bad happened, like appendicitis, in the interval time period, you know, we physicians are paranoid.
“So, instead, we do the CT scan, we do the lab work, and when nudged by some marginal other lab results, we did an ultrasound. We got through weeks’ worth of workup and bypassed prior auth in one afternoon. Multiply this same thought process many, many times over. I actually saw three patients who would fit in this general bucket today. That phenomenon is common. You can see where the explosion of acuity and visit volume comes from.”
This echoes, by the way, what Mick Connors, MD, wrote on LinkedIn the other day. He wrote, “The fact is, primary care has so few resources these days, not much can be offered. There’s no X-ray, lab, procedures, RNs, mental health, etc. And more fees for quicker services and no penalty for sending everyone to the ER. So, it’s all built into the fee-for-service system.”
And you see that in the data, everything above. There’s loads of it that corroborates that differences in healthcare access, principally primary care access, is a huge determinant of the volume and the average price of ER visits.
It’s a little bit ironic that the bigger driver, it seems, is the lack of urgent care and primary care that’s driving ER trends, not their existence.
Al Lewis gives advice for what plan sponsors can do about these rising ER charges in the show that follows. You’re going to want to listen to him explain them, but the first is help your employees who are trying to sue a hospital for egregious charges.
You both are on the same side here. So that’s number one. Secondly, educate members about consent forms. And we talked about this one at length in the earlier show with Al (EP386), so do go back and listen to that if consent forms, even just that language, is unfamiliar to you. Then lastly, be proactive about these rates that you may get charged as a plan.
And Al has a bunch of advice here (again, towards the end of the show) on how to do that.
So, here’s my conversation with Al Lewis, who is CEO and founder and “quizmaster in chief” over at Quizzify. Contact him, for sure, for more on any of this. He says every time he makes an appearance on Relentless Health Value, lots of people call him—so, you won’t be the only one.
Also mentioned in this episode are Brian Cotter; John Lee, MD; Mick Connors, MD; Quizzify; Rob Andrews; and Vivian Ho, PhD.
You can learn more at quizzify.com and by emailing al@quizzify.com. You can also follow Al on LinkedIn.
Al Lewis wears multiple hats, both professionally and also to cover his bald spot.
Hat #1: Employee Health Literacy. He is the founder and “quizmeister-in-chief” of Quizzify, whose mission is to help companies teach their employees to utilize health care services appropriately, using a format best described as “Jeopardy meets Choosing Wisely meets Comedy Central.” Quizzify is the only vendor authorized to display the Harvard Medical School “Veritas” shield and has received excellent reviews from users.
Quizzify is also well known for its ER Sticker Shock Prevent Consent, which has been endorsed by Dr. Marty Makary and Dave Chase, among others. It can be taped to an insurance card, used as a stand-alone card, or downloaded into your Apple or Google Wallet and will “pop up” when you enter an ER. It limits ER bills (both in- and out-of-network) to 2x Medicare, which is less than half of most “negotiated” rates.

His quiz-specific background includes authorship of the best-selling Newsweek Presents the Ultimate Trivia Game, which Games magazine lauded as having the best questions of any trivia game; hosting two quiz shows on Boston network affiliates; and appearing on Jeopardy.
Hat #2: Outcomes Measurement. As an author, his critically acclaimed category best-selling book on outcomes measurement, Why Nobody Believes the Numbers, chronicling and exposing the innumeracy of the health management field, was named digital health book of the year in Forbes. Cracking Health Costs, written in conjunction with Walmart alum Tom Emerick, was also a trade best seller.
He was the co-founder of the World Health Care Congress’s Validation Institute.
His expertise in outcomes measurement got him named one of the unsung heroes changing healthcare forever.
He graduated Phi Beta Kappa with honors from Harvard, where he taught economics as well. He also graduated from Harvard Law School, albeit with no honors that time—other than winning their annual trivia contest, of course.
08:32 What is going on in ER visits, and how big of a deal is the total spend?
10:16 Why is the price of ER visits going up when it should be going down?
11:59 What is the major source of unexpected medical debt?
13:27 What is code creep, and why is it happening?
16:26 Why are plan sponsors unable to negotiate emergency room services?
25:53 Why is it important not to agree to consent when you go in to visit the ER?
31:28 What steps can plan sponsors take to be proactive about limiting ER spending for their employees?
Recent past interviews:
Click a guest’s name for their latest RHV episode!
Betsy Seals, Wendell Potter (Encore! EP384), Dr Scott Conard, Stacey Richter (INBW42), Chris Crawford, Dr Rushika Fernandopulle, Bill Sarraille, Stacey Richter (INBW41), Andreas Mang (Encore! EP419), Dr Komal Bajaj
[00:00:00] Episode 464 ER Emergency Room Visits Now 6% of Total Plan Spend. Is It Upcoding or What? Or What Indeed? Today I speak with Al Lewis.
[00:00:22] American healthcare entrepreneurs and executives you want to know, talking, relentlessly seeking value.
[00:00:30] Today I am speaking with the one, the only Al Lewis and we're gonna talk about how 6% of a lot of plan sponsors total spend is now going to ER, ED, Emergency Room Emergency Department visits. That's a lot of spend. Al digs into this so I'm just going to gloss over it all and make my own points or two along the way. I am sure here as the intro.
[00:00:56] But the reason why ERs are costing so much these days is number one, because ER volume nationwide is in fact trending up, i.e. more patients are going to the ER. We had a pandemic in the mix, so it's a little sketchy to track. But yeah, the volume of ER visits per capita seems to be increasing and it's increasing faster than the population. And number two reason, at the same time, the average cost per visit is going up.
[00:01:22] So there's a bunch of things that I'm going to say today where if you want to dig in on them, go over to the show notes. But volume is going up. Also, the price per visit is going up. Let's linger a little here on the price per visit part of the equation. The average cost per visit went up 15% in 2023, which is something that Al brings up in the conversation that follows in a little bit greater depth. Now, in the context of ER visits becoming more expensive, here's a common question that gets posed.
[00:01:51] Is this increased cost because option A, ER visits are being upcoded or option B, are patients showing up in the ER actually sicker? Now, I do realize that is an either or, and most of us listening today, and also many who pose this question, and certainly Al Lewis, are fully aware that there is other stuff going on. But let's just keep it simple with this either or binary before we make it more complicated.
[00:02:20] So are ER visits being upcoded or are patients sicker? There is a right answer to that question, by the way, although not everyone wants to hear it. So let us begin with, it is a verifiable fact that visits are being coded at higher acuities than in the past. And the higher the coding acuity, the more the ER visit is going to cost, just to state the obvious. That's why there is a financial reason to upcode because the higher codes have higher associated prices.
[00:02:49] Brian Cotter on LinkedIn the other day cites an ER coding analysis, and Al Lewis sent me a KFF, Kaiser Family Foundation slide, basically showing the same thing. ER visits are being coded at higher acuity. Links in the show notes to both of these graphs, but it all boils down to, as Brian put it in that LinkedIn post, a notable shift toward higher intensity coding in physician billing.
[00:03:14] So codes are upped, but are the patients actually sicker, thus warranting the higher acuity codes? Again, is there an increase in actual patient acuity or is it just a change in coding practices jacking the codes up to higher severity levels? Let me leave you on the edge of your seat just a moment here while I tick through some of the proposed answers to this question, whether patients are sicker, thus requiring higher levels of coding acuity.
[00:03:40] You will certainly get some folks very, very definitely with three underlines talking about their premise that urgent care has siphoned off most of the low acuity cases that were going to ERs in the past, which has left hospital ERs with higher acuity cases. So there is certainly a crew who is firmly in the yes, patients are actually sicker camp. Is this actually true? As per the data that sicker patients are showing up in the ER? Well, no. Not that I could find.
[00:04:09] And if you have stat showing otherwise, certainly send them over. I did, however, find a KFF Health News examination of physician upcoding, which found that minor procedures such as removing a splinter or treating a wart are increasingly being billed as surgery, costing hundreds of dollars. Then I asked Al Lewis whether there's evidence of higher acuity patients showing up because urgent cares are dealing with the easy stuff. And he wrote me back with references.
[00:04:36] He said if visits were actually higher acuity, then you would see a commensurate increase in hospital admissions aligned with that acuity. If, on the other hand, upcoding was the cause of more level four and level five visits like the KFF Health News examination revealed, then you would see a reduction in admissions to the hospital from those codes.
[00:05:00] And that is apparently what happens quite dramatically in California where it was actually studied. Details in the show notes showing way lower hospital admissions from the way higher acuity codes. So, yeah, upcoding. And number two reason ERs are costing so much these days. Again, ER volume nationwide is, in fact, trending up.
[00:05:22] And a third issue that Al talks about for ER total spend becoming more expensive is just it's really, really difficult for plan sponsors to negotiate for ER services. They are emergencies. Nobody can navigate. A fourth factor that Al Lewis talks about in the show that follows is some shifts in what has been going on for in-network patients since the No Surprises Act. And, again, we take that up in the conversation that follows.
[00:05:48] So four factors underpinning the rise in emergency room spend. But there's kind of an underlying dynamic here that I want to bring up. And it's kind of interwoven through a lot of the conversation. I want to quote Dr. John Lee, who is, in fact, an emergency room physician. When I gave him kind of the run of show on this episode, Dr. John Lee said to me, Here's an anecdote from today. I just saw a young patient with abdominal pain.
[00:06:15] She has had symptoms on and off for months and has had little progress getting any attention from her primary physician. I could theoretically do some screening and labs and then have her scheduled for an office recheck tomorrow. But I had zero faith that she will actually get in to the office in follow-up. Also, even if she did and something bad happened, like appendicitis in the interval time period, you know, we physicians are paranoid.
[00:06:41] So instead, we do the CT scan, we do the lab work, and when nudged by some marginal other lab results, we did an ultrasound. We got through weeks worth of workup and bypassed prior auth in one afternoon. Multiply the same thought process many, many times over. I actually saw three patients who would fit in this general bucket today. That phenomenon is common. You can see where the explosion of acuity and visit volume comes from. This echoes, by the way, what Dr. Mick Connors wrote on LinkedIn the other day. He wrote,
[00:07:11] The fact is primary care has so few resources these days, not much can be offered. There's no x-ray, lab procedures, RNs, mental health, etc. And more fees for quicker services and no penalty for sending everyone to the ER. So it's all built into the fee-for-service system. And you see that in the data, everything above. There's loads of it that corroborates that differences in health care access, principally primary care access, is a huge determinant of the volume and the average price of ER visits.
[00:07:39] It's a little bit ironic that the bigger driver, it seems, is the lack of urgent care and primary care that's driving ER trends, not their existence. Al Lewis gives advice for what plan sponsors can do about these rising ER charges in the show that follows. And Al has a bunch of advice here, again, towards the end of the show on how to do that.
[00:08:04] So here's my conversation with Al Lewis, who is CEO and founder and Quizmaster-in-chief over at Quizify. Contact him for sure for more on any of this. He says every time he makes an appearance on Relentless Health Value, lots of people call him. So you won't be the only one. My name is Stacey Richter. This podcast is sponsored by Aventria Health Group. Al Lewis, welcome back to Relentless Health Value. Well, thank you for having me back. It is a pleasure to have you back, my friend.
[00:08:31] I'd love to talk with you about what is going on in emergency departments, emergency rooms, EDs, ER, because this is fast becoming a topic. How big a deal is this right now? Well, in terms of total spend per belly button, it's about 6%, which may not seem like a lot. But if you break everything down, 6% is more than everything except for drugs and inpatient.
[00:08:59] So 6% of total spend or 6% of like hospital spend? It's 6% of total spend. For most plan sponsors. For most plan sponsors, yes. The rates are now well over 200 visits per thousand in the commercially insured population, which means the average person under 65, not insured by Medicaid, is going to the ER once every four to five years, which seems like a lot. And yet that's the statistic.
[00:09:25] Paradoxically, despite the proliferation of urgent care, this number has been growing. And also despite the fact that the copays are going up. Okay. So the situation writ large here for plan sponsors, probably seeping into Medicare to a certain level, but as you said, not Medicaid. We're taking them off the table now. But what we've got is the average member, plan member, is going to the ER once every four to five years.
[00:09:51] Therefore, that results in if anybody looks across their membership, you're going to have 200 out of 1,000 who have showed up that particular year in the ER, resulting in ER spend being cumulatively about 6% of any plan sponsors' total costs in any given plan year. That's the summary. The average plan sponsor in the ER, yes. Is this trend increasing? Like was it 2% a couple of years ago and now it's 6% or are we holding steady here?
[00:10:21] The volume is going up and the prices are going up. It actually, if you take the price for any given visit and the number of visits, the total went up by 15% in 2023 when it should have been going down because that's after the No Surprises Act. And I have to say the data is only public sector data. That's the only data for government entities that's been accumulated.
[00:10:44] And it's probably also true that private sector has slightly less than 200 visits a year, whereas the public sector is somewhat more. So I'm averaging it to 200 in small change. So we've got a multivariate increase. Yes. Despite the fact that there's urgent care, which is kind of interesting, plan members, they're going to the ER despite the fact that there are urgent cares. And the prices of those emergency room visits are going up. Yes.
[00:11:12] And I have a theory for the urgent care thing. And unlike everything else I'll talk to you about, it's not data. But I believe there's some short staffing issues. So at least in our area, urgent care is ironically not open on weekends. So I've had personally two situations where I went to urgent care, found out it was closed for something that did not need an ER visit and had to go to the ER. So it's almost like urgent care has become primary care.
[00:11:39] Because primary care, there's so many areas of the country where you wait eight months to get a visit right now. Yes. And in fact, that was the other theory, Stacey, is that people simply cannot get not just urgent care, but primary care. So that's why the ER visits are going up. I mean, what's incontrovertible is that they're going up. Emergency room volume is going up as well as the price of an average visit is going up. So for plan sponsors, we have a situation there.
[00:12:06] But then if you're thinking about this from a patient finance, from a member finance perspective, at the same time, we also have medical debt, which I understand is increasing. And a lot of that is due to ERs as well. Yes. And in fact, the major source of medical debt are these unexpected visits. These things create considerable financial hardship, especially for people who are on high deductible plans.
[00:12:29] Even if you have $4,000 in the bank, one ER visit in network can cost the whole $4,000. Other care settings are not readily available. Someone winds up in the ER. It's easy to get a $4,000 bill in the ER. And 41%, I think was the last stat I saw, 41% of Americans have medical debt. So if you've got 200 out of 1,000 in the ED every year, you can kind of see how those numbers get where they are.
[00:12:59] As well as just, you know, if you're going to the ER every time you have a diabetes exacerbation. The mission of the emergency room is to make your emergency not an emergency, not ensure that you've got continuing disease management or anything like that. So why is this happening? Which is causing the increase of prices in the ED. Well, number one would be the upcoding. I have a chart and I'll send it to whoever wants.
[00:13:27] It only goes through 2021, but that shows there are five codes in the ER from 99281 up to 99285 that over time, the 99284s and 5s that used to be the minority are now the significant majority. And I can tell you that most of that should not be done and they're not being caught. There are different codes that the emergency room uses, as you said, from 99281 to 99285, right?
[00:13:54] So there's five different severity codes from level one visit, which is pretty much just like something really, really simple to five, which is gunshot wounds, right? You had been telling me about a recent ER visit that your wife had. She suspected she had Lyme's disease and ultimately her visit was coded as a level four. Like she's one down from a gunshot wound.
[00:14:16] So the point is prices are going up because if the ER upcodes the severity of the reason why the person is in there and the type of care that they received, then the dollars start going up. So if everybody who in the past would have been coded as a one or a two or even a three now all of a sudden is a four or five. Yeah, that's not rocket science. Yes. And I could give you many examples of that.
[00:14:42] My favorite one was once again, just the other day, another client, the daughter fell and she did actually briefly lose consciousness. So they went to the ER quite appropriately. This was 11 at night. So the mother and the daughter stayed till about 730 in the morning. At that point, urgent care is opening. So they say, well, we'll just go to urgent care because we really want this to be seen. So they leave the ER and go to urgent care without being seen in the ER. And they got a bill for $1,000 from the ER.
[00:15:11] So it's kind of like a zero level code visit and they're still getting $1,000. Yes. They said, well, we triaged you. They said you left against medical advice. And our argument was any good doctor would tell you to go get seen somewhere, you know. So good medical advice would have said, yeah, by all means, go get seen. There is significant code creep across the country.
[00:15:29] If you put that together with the other thing, Stacey, about how people are going to the ER for little things because they can't get in to see their other doctors, there should actually be many more 1s, 2s, and 3s, not more 4s and 5s. Okay. So the first reason why we're seeing this trend up of now ER visits or 6% of plan sponsor costs on average, one of them is just this code creep.
[00:15:53] That even if the volume were remaining the same, which that's also going up, but even if it were remaining the same, we would have an increase in spends because the prices of an average visit are increasing. So number one, we've got code creep up coding. Number two, volume is actually going up. Anything else? Number three is, frankly, because they can. The thing about ER is there are two things about it.
[00:16:19] One is it's very, very difficult, if not impossible, to negotiate an ER price for an employer based on volume because you can't direct people to ERs. You can negotiate a price for joint replacements or normal deliveries or that kind of thing. But ER is what you get. And number two, their ability, the provider's ability to negotiate with the payers is paramount.
[00:16:45] They're holding all the cards because you need them in their network. And they also say that unlike in the electives, in electives it's common to get 120% of Medicare. In the ER, they're saying, well, we have to cover all the uninsured people. So we have to charge you more in order to cover the cost of people who don't have insurance. And that creates some very interesting dynamics. So in Maryland, for example, where they have a every penny pays the same price. ER visits are still in the three figures.
[00:17:16] It's unbelievable how low they are. Number two, Massachusetts, which is known for high health care costs, has like the fifth lowest ER costs because everybody is insured. So the hospitals can't pull that thing. Meanwhile, on the other end of the spectrum, you've got Florida, where it's literally seven or eight times what Maryland is. So the third reason that you're giving for this trend line is ER. It's like squeezing a balloon, right? And there's a weak spot in the balloon for ER.
[00:17:44] As you just said, if it's something that's elective, plan sponsors have an opportunity to get in there and negotiate. But if you're talking about an emergency visit, then patient's going to go to the ER if they feel like they're going to need, they're having an emergency. So it's hard to negotiate emergency room services as the first part of the because they can.
[00:18:06] The second part is that there seems to be a very intuitive reason for a hospital negotiating for higher ER visits just because it's exactly the same care setting that all of the uninsured patients are also winding up. So, you know, you can in a very clear way probably pop up a PowerPoint slide and show that the plan sponsors in the area need to cover the uninsured patients in the area.
[00:18:35] And anyone who's community minded is going to be sympathetic there. But, you know, plan sponsors, you're paying for all the uninsured people, allegedly, at least. Yeah, here's the interesting thing about that, Stacey, is that in the old days, you could actually do, they called it a wallet biopsy. When someone came into the ER, if you didn't like their insurance, you could just send them somewhere else. And the government very wisely, and I might add totally bipartisanly, put the kibosh on that, you know, at this point almost 40 years ago.
[00:19:04] And that's when the ER prices started creeping up because that's when the hospital said, we got to cover everybody. And it's only gotten worse since then. And I certainly would suggest that anybody who's kind of thinking about that point that just got made, that plan sponsors are very clearly paying for, in a way, the health of the community. To listen to the show with Rob Andrews, who really gets into this, especially relative to maternity and maternity outcomes.
[00:19:29] Okay, so we've talked about three reasons for the increase in this growing trend line for ER spend up to now 6%. We've got just increased volume. We've got this code creep that you talked about. You've got the because they can. This is certainly an easy way for a hospital who's looking to increase their revenue to do so without a ton of pushback. Do we have a number four here? Yeah, so the No Surprises Act has worked pretty well.
[00:19:56] The headline making ER visits, you know, the $10,000 COVID test, they are all gone. So, you know, kudos to the bipartisanship behind that. But it's like the balloon in that the greatest abuses are now taking place in network. And they're not headline makers. They're just every one of these is higher. You see a lot more scans and a scan in an emergency setting costs thousands of dollars.
[00:20:24] So it's not only the number of patients that are showing up. It's now that when the patients do show up beyond the code creep, which is just the visit itself gets coded higher. It's also that there's now more stuff that's being done in the ER, like more scans. It appears, and I cannot give you chapter and verse on this, but it appears that considerably more scans are being done. I mean, the United States has always been high in scans.
[00:20:52] In fact, we do, and this one I do have the stats on, we do twice as many scans, both CAT scans and MRIs, as the average country in the Organization for Economic Cooperation and Development, the OECD, with no better outcomes, with worse outcomes. Now, the thing about the ones in the ER is the same scan that would cost $400 or $500 outpatient is costing $4,000 or $5,000 inpatient. And then it gets, quote unquote, discounted by the carrier's negotiation down to $2,500.
[00:21:21] So if we're thinking about the number four reason for this increased ER trend since the No Surprises Act, so you definitely could probably track it back to some finance person who's like, wait a second, we're going to lose the million dollar heart attack. So how are we going to make that back one patient at a time? We generally speaking, and this is their exceptions like Walmart and Caterpillar, but generally speaking, the larger the employer, the less they connect the dots, basically, and they just write a whole bunch of checks.
[00:21:48] Yeah, I was talking to a large plan sponsor the other day who might have disagreed with you. I think he would say that it's not necessarily the size of the employer that matters. It's a combination of their philosophy and then also their member mix. He said something really interesting. He was like, as a plan sponsor, you got to choose. Do you want to have a well-priced plan and save money or not? He's like, that's the first choice you have to make. Like, pick one.
[00:22:17] And if you choose not to, like maybe you've got all tech employees who are making $179,000 a year and who you think don't care whether they pay $4,000 in the ER. They can afford it. So, you know, I think there's probably a lot of stuff that's going on there. Okay, so we have talked about four things here that can accelerate this trend line with ER.
[00:22:43] The last one was stuff going on with the No Surprises Act that increases in-network spending per patient. So it's not just the volume of patients that's going up. It's what's happening to them once they show up. Are we capped at four, Al? If there's a fifth, it would be minor. So I would say that the first three are, you know, 80%. The last one is 10. And then everything else combined would be 10. So let's get into the advice portion of the pod now.
[00:23:12] And I'm just going to stick in here that one of the reasons you can fight and you can win. Like, because of the upcoding, there's a precedent that doesn't want to get set here. So you can get a write-off as a plan sponsor if you take the time to ask for it and state the facts. Yeah, but there's a key thing here.
[00:23:39] The key thing is you cannot agree to their consent when you go in. If you agree to their consent when you go in, you have to sign twice. Once to get treated, you've got to sign that. And then once I agree to get paid or I agree to pay whatever you want. Well, there's a reason for that second thing being, signature being different from the first, is that you don't have to agree to it. And according to the Emergency Medical Treatment Act, they have to treat you exactly the same, whether you agree to it or not.
[00:24:07] Now, if you agree to it, you've seriously limited your options. And you do have options, and we'll talk about them later. If you disagree with it and you write in your own consent or you stick on a sticker that has a consent or your insurance card has a consent that says that you only agree to appropriate treatment coded at the correct level at X times Medicare, like 200% of Medicare. You know, if you're a huge organization, maybe 150% of Medicare.
[00:24:35] And they will 95% of the time just accept it. They'll have no idea what's going on, and they'll accept it. If they've done that, you will win. And you will get, now Medicare, you know, people will talk about, you know, how good or how bad it is. One thing they're extremely good at is limiting pricing in the ER. So even if you multiply it by two, you're still paying a low price. So, okay. So it really is at the member level.
[00:25:04] That because if a member goes in and every time the iPad gets shoved in their face, they squiggle their name on the dotted line. If that is happening, what that patient just did is financially committed themselves to basically pay whatever the bill is. There is some recourse, good recourse for some people at a certain income rate. But basically, you're limiting your options very significantly. Got it. Okay. And we did a whole show about this. I will link to it in the show notes.
[00:25:33] So if somebody is interested in a deep dive into the consent form, please go back and listen to that earlier show because we're not going to get into it here. The one thing I would note, which is different from the earlier show we did on the consent, is that there are ways of actually automating the consent. So you don't have to rely on the patient, on the employee to put a sticker on or to remember what to do or anything like that. It's actually fairly ingenious. And you can do it on your own if you want. Frankly, it's easier if you do it with us.
[00:26:01] But you write to the hospital in advance and you say that anybody who comes in under this account number, here's the consent that we agree to pay. And if they don't object, that's what you pay. And it's not quite that easy. And on the card, you have to then put a little sticker. The employee doesn't have to do anything. But on the card, it says, see consent on file. And then there's a QR code that takes you to this email where the hospital has agreed to this.
[00:26:30] Now, it is possible the hospital will write back and say, we don't agree. It's extremely unlikely because it's, well, number one, it's never happened. But number two, when you send this to the hospital, I don't know if you've noticed this, but hospitals make themselves impossible to contact electronically because they don't want to set up audit trails. So what you need to do is go to ZoomInfo or some other way and find a few emails from the hospital and send this thing to them and say, sorry, we didn't send it right to the ER billing because we didn't have their email. So please go ahead and forward it.
[00:27:00] If they don't forward it, that's on them because it's well-established in law that you cannot murder both your parents and ask the court for sympathy because you're an orphan. It's called estoppel. If they make themselves impossible to contact, they can't complain that you didn't contact them correctly. Okay. So part A to this as a plan sponsor is do the work ahead of time. Find the hospitals that your members are likely to show up at in an emergency and send them all. A, this is what we consent to in advance. So that's part A to this.
[00:27:30] But then again, part B, as you have mentioned is if there is an egregious bill, then the member needs to send it to you, plan sponsor, so that you can turn around and say this is ridiculous. Right. But let's talk about the situation where somebody does not do that for people who are under $95,000 to something like that. And they do get the bill.
[00:27:53] The hospitals have, it's called a 501R charity, well, they call them financial assistance or charity care that they're not telling you about. And we run into these things all the time where hospitals or doctors have a much better way of doing something that's much less expensive that they don't tell you about. These hospitals have, if they're nonprofit, they have to provide a certain amount of what they call charity care. All you got to do is ask for it repeatedly because they're not telling you about it.
[00:28:22] And we've got all sorts of memos on this where someone is trying to fight our fight. And they say, well, you know, the patient does can get financial assistance, but they don't offer that up front. You got to really know what you're asking for. So as a plan sponsor, that would be number two. If the plan member or the plan member themselves, right? If the plan member is making less than $95,000 a year, then also go back to the hospital and get the charitable dollars, which are available.
[00:28:48] And again, if a hospital that is taking Medicare and Medicaid has been paid by the federal government, then they are subject to the 501R rules there. Yeah, I think it's only nonprofits, but it might vary by state. And the cap also varies by family size, but it's always worth looking into even if you're under $120,000. So we got one part A and part B that you have to ensure that your consent is modified up front.
[00:29:18] So there's a proactive bit to this, but then reactively, if a member does get an egregious bill, then turn around and help them fight it. I mean, and this, if you start thinking about the fact that everybody is paying a whole lot of money for insurance, and then a plan member finds out the hard way that they're basically functionally uninsured and gets, I'm going to say, taken advantage of in the provider setting,
[00:29:43] then their trust in this whole operation and in their employer plan really diminishes and just take to the social media if you want to see that happening over and over and over again. And then number two, as a nonprofit, the hospital does have to offer charity care. So if it is available, they generally speaking, I'm going to say, and there's New York Times articles about this. So generally speaking, the patient is not necessarily informed early and often about the fact that that charity care is available.
[00:30:13] So yeah, let's be a little more specific. They are not informed. They have to proactively ask for it. They're not informed. And I do just want to emphasize the fact that you do no longer have to rely on the employee for these consents. You can, there's precedent for sending these to the hospital in advance. So if you do these things, if you inform your employees, if you are willing to fight, if you send the consent in advance,
[00:30:39] and if you make sure you use it, there are vendors, not Quizify, so I can mention them, but Full Health, Good Bill. There are probably others that will manage this 501R thing for you. If you do all these things, your own ER spend should be falling. And certainly your employees, the last thing you want them doing is going bankrupt on your nickel, not just for their own sake, but because guess what? They're not going to be engaged at work anymore. So you got in your own best interest. For sure.
[00:31:06] Al, if someone's interested in learning more about the work that you're doing, where would you direct them? I would say al.quizify.com or www.quizify.com. We're very easy to find. And, you know, it doesn't take long to set this up. You can implement this stuff in an hour. Al Lewis, thank you so much for coming on Relentless Health Value today. I'm always glad and thank you for having me on. Hi, this is Al Lewis. So thank you very much to everybody who listened to the entire podcast.
[00:31:34] I hope you learned something useful, as I always do when I work with Stacey.