
The show today is a recording of an earlier conversation between Abby Burns and myself. This original conversation happened during the Raising the Value Bar Summit, which was a summit all about value and the what, why, and how of it all.
For a full transcript of this episode, click here.
If you enjoy this podcast, be sure to subscribe to the free weekly newsletter to be a member of the Relentless Tribe.
Abby asks me questions like why did I start the podcast, which fits the value theme because this show is entitled Relentless Health Value, after all.
I get asked how I define value. Fair question. Also, trick question, because value is in the eye of the beholder. All any of us ever have is a capability, a capacity.
The sorcery by which any given capability transmogrifies into value happens when somebody else’s problem or pain or need or want is solved for by said capability. Oh, you thought that was the tricky part? No, not in the healthcare industry. That’s probably the easy part, which is saying something, because product market fit is never easy.
The tricky part here is that in healthcare, as I’ve often said and heard, healthcare is an industry where one person eats the dinner, somebody else orders the dinner, and a third person pays for it. So, the patient may see immense value in whatever it is that somebody’s doing. But if the orderer and the payer don’t, well, the capacity is going to remain a caterpillar that never turns into a butterfly, most likely.
Said another way, the tricky part in healthcare is if you don’t create win-wins across a bunch of different boards, value won’t be realized for patients. And the problem with that is the number of zero-sum games we have afoot around here in the healthcare industry, which make this really difficult.
Before we kick into this show, I just want to mention, because it comes up several times in the conversation that follows, there was a talk by Daniel Kuzmanovich, who is managing director and expert partner over at Advisory Board. Daniel had given a talk earlier during that same value summit, and during this talk, he mentioned the idea that when measuring value in healthcare, there’s four tensions.
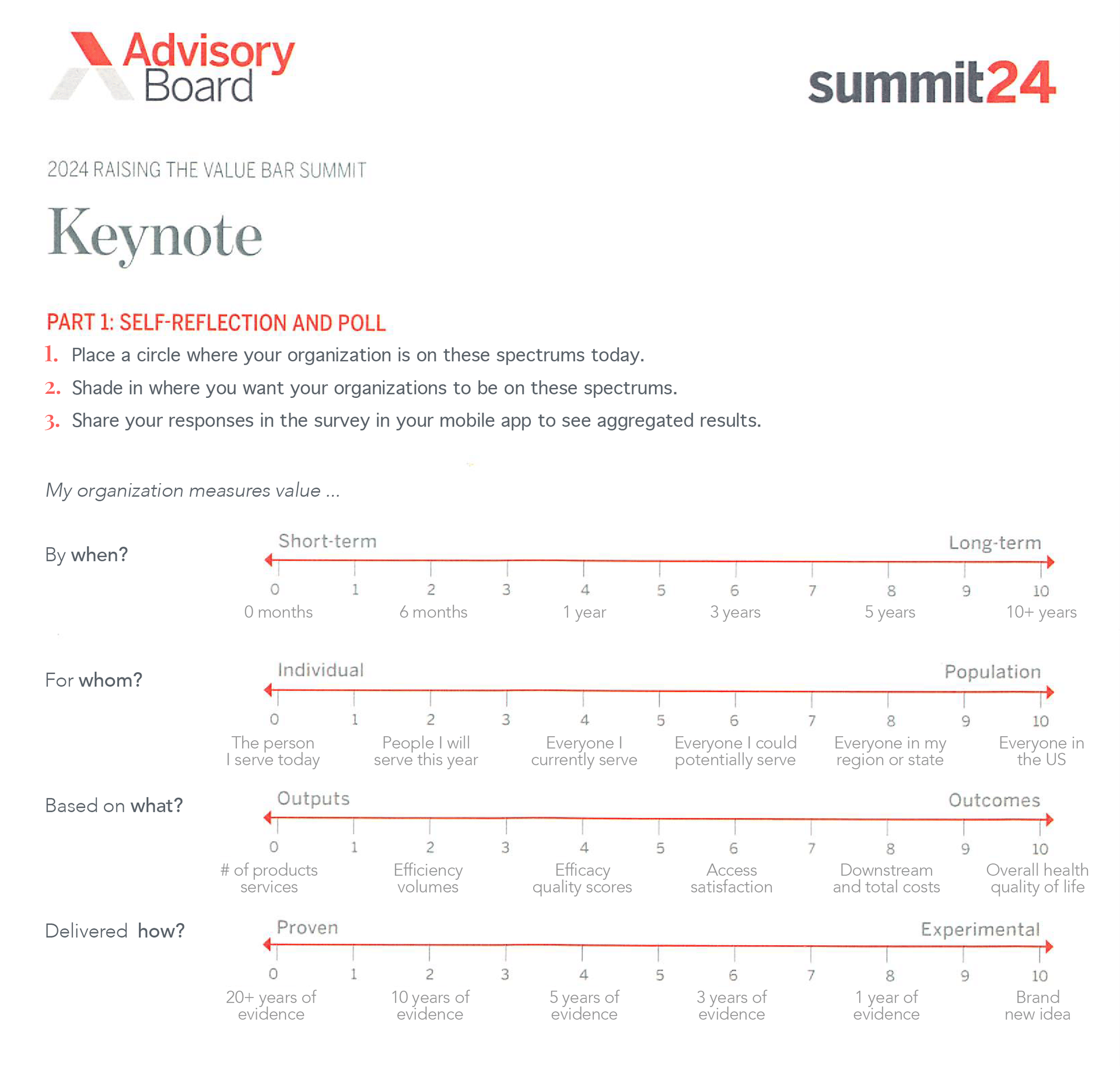
And if different stakeholders (or different people, actually, even within one stakeholder) have different perspectives on how value is created in light of these tensions, yeah, that’s where spheres collide and value drains away, never to be realized. So, the four tensions are:
Value Tension 1—When: By when must the value be realized? And some say that there is a tension between short-term value creation and long-term value creation. So that’s the first tension, this tension between somebody trying to get something done quick in the short term or only concerned about the short term and then what then happens in the long term.
Value Tension 2—Value for Whom: We could define this a bunch of different ways, but how Daniel defines it is the tension between individuals who are thinking one patient at a time and those who are thinking in terms of populations—could be populations of an organization; it also could be nationwide populations. Like, if I’m a doctor, do I worry about patients singularly or individually versus somebody thinking more top down from the population level down?
Value Tension 3—Value Based on What: And this tension could be, Are we thinking about value of the output, or are we thinking about the value of the outcome? Again, you’re gonna go about things kind of different ways if you’re thinking about output value versus if you’re thinking about outcome value. And, for sure, there could be tension if there’s not alignment there.
Value Tension 4—Proven or Experimental: People who only want to do things that are proven to drive value versus those who might be up for some experimental stuff. So, there’s this kind of tension between offering proven value and focusing on only things that are proven and evidence based versus those who are looking to incorporate experimental things into what they’re doing.
So, the tensions are when, short term, long term; for whom, patients or populations; based on what; and then lastly, is it proven or experimental?
Before we roll tape, I just want to thank Abby Burns, who is my interviewer today and a great one at that. She even managed to keep the likes of me mostly on track and on topic, which is no small feat. Thank you so much, Abby.
Abby Burns is an expert partner over at Advisory Board. She’s also a frequent host on the Radio Advisory podcast and a strategy lead.
Also mentioned in this episode are Abby Burns; Daniel Kuzmanovich; Scott Conard, MD; John Lee, MD; Mike Tuggy, MD; and Michael Leavitt.
For more information, go to Radio Advisory or Aventria Health Group.
Abby Burns is a researcher and facilitator with Advisory Board and serves as co-host of the Radio Advisory podcast. Through leading research and connecting with healthcare leaders both live and via Radio Advisory, Abby aims to provide meaningful thought partnership to help stakeholders across the industry to improve healthcare within and across their own domains. A self-avowed “healthcare generalist,” Abby’s research has a home base in health system strategy. She has previously led research on behavioral health, rural health, population health management (including primary care strategy and social determinants of health [SDOH]), and more.
Abby previously volunteered as an EMT in Prince George’s County, Maryland, where she regularly witnessed many of the challenges Advisory Board research aims to help members address. She earned her BA in public health from the University of Richmond.
Stacey Richter uses her voice and thought leadership to provide insights for healthcare industry decision makers trying to do the right thing each week on Relentless Health Value. Each show features expert guests who break down the twists and tricks in the medical field to help improve outcomes and lower costs across the care continuum. Relentless Health Value is a top 100 podcast on iTunes in the medicine category and reaches tens of thousands of engaged listeners across the healthcare industry.
In addition to hosting Relentless Health Value, Stacey is co-president of QC-Health, a benefit corporation finding cost-effective ways to improve the health of Americans. She is also co-president of Aventria Health Group, a consultancy working with clients who endeavor to form collaborations with payers, providers, Pharma, employer organizations, or patient advocacy groups.
03:33 Stacey’s journey and mission.
04:16 The story of Scott Conard, MD (EP391).
09:28 Why it’s important not just to drive change but to sustain it.
12:23 Heart Failure: A Case Study in Value.
14:13 EP438 with John Lee, MD.
15:07 Why patient positive value often fails instead of succeeds.
18:07 How financial toxicity has become clinical toxicity in healthcare.
19:44 How cultural norms have evolved into healthcare challenges.
23:38 The story of Mike Tuggy, MD, in Washington.
25:13 Looking at the four tensions in measuring value as continuums.
25:37 Why timeline is important in creative value in healthcare.
27:52 Finding Allies by Michael Leavitt.
28:34 What are the four ways to measure value in healthcare?
29:27 How do payers and providers collaborate to align on value metrics?
31:26 Why will proven versus experimental treatments become more important in the next few years?
34:54 Stacey’s manifesto (EP400) and values for personal integrity in healthcare.
38:55 Stacey’s parting advice.
Recent past interviews:
Click a guest’s name for their latest RHV episode!
David Muhlestein, Luke Slindee, Dr John Lee, Brian Klepper, Elizabeth Mitchell, David Scheinker (Encore! EP363), Dan Mendelson, Dr Benjamin Schwartz, Justin Leader, Dr Scott Conard (Encore! EP391)
[00:00:01] Episode 441, Tables Get Turned. This is me interviewed by Abby Burns from Radio Advisory about what is value. American healthcare entrepreneurs and executives you want to know. Talking. Relentlessly seeking value. The show today is a recording of an earlier conversation between Abby Burns and myself.
[00:00:37] This original conversation happened during the Raising the Bar Summit, which was a summit all about value and the what, why, and how of it all. Abby asks me questions like, why did I start the podcast?
[00:00:51] Which fits the value theme because this show is entitled Relentless Health Value after all. I get asked how I define value. Fair question. Also trick question. Because value is in the eye of the beholder. All any of us ever have is a capability, a capacity.
[00:01:08] The sorcery by which any given capability transmogrifies into value happens when somebody else's problem or pain or need or want is solved for by said capability. Oh, you thought that was the tricky part? No, not in the healthcare industry.
[00:01:23] That's probably the easy part, which is saying something because product market fit is never easy. The tricky part here is that in healthcare, as I've often said and heard, healthcare is an industry where one person eats the dinner, somebody else orders the dinner and a third
[00:01:38] person pays for it. So the patient may see immense value in whatever it is that somebody's doing. But if the orderer and the payer don't, well, the capacity is going to remain a caterpillar that never turns into a butterfly most likely.
[00:01:55] Said another way, the tricky part in healthcare is if you don't create win-wins across a bunch different boards, value won't be realized for patients. And the problem with that is the number of zero-sum games we have afoot around here in the healthcare industry, which make this really difficult.
[00:02:14] Before we kick into this show, I just want to mention because it comes up several times in the conversation that follows, there was a talk by Daniel Kozmanowicz, who is managing director and expert partner over at Advisory Board.
[00:02:27] Daniel had given a talk earlier during that same value summit. And during this talk, he mentioned the idea that when measuring value in healthcare, there's four tensions. And if different stakeholders or different people actually even within one stakeholder
[00:02:42] have different perspectives on how value is created in light of these tensions, yeah, that's where spheres collide and value drains away never to be realized. Before we roll tape, I just want to thank Abby Burns, who is my interviewer today and a great one at that.
[00:03:00] She even managed to keep the likes of me mostly on track and on topic, which is no small feat. Thank you so much, Abby. Abby Burns is an expert partner over at Advisory Board. She's also a frequent host on the Radio Advisory podcast and a strategy lead.
[00:03:15] My name is Stacey Rixer. This podcast is sponsored by Eventria Health Group. Stacey, I'm so glad that you could be here this morning. Well, I am so glad to be here also.
[00:03:23] Stacey, I know a lot of folks here and certainly a lot of Radio Advisory listeners are intimately familiar with you and with Relentless Health Value. But for those who might not be, can you give us a little bit of background?
[00:03:34] What is the goal of Relentless Health Value and what made you see the need to create a space like that? Relentless Health Value has been around for 10 years now. We started in 2014, but the original goal, which remains the original goal, the goal,
[00:03:50] is to equip those who are looking to transform and fix healthcare with the information that you need about what's going on with other stakeholders to ensure that you can actually succeed without encountering a series of unfortunate events. Certainly no shortage of need there.
[00:04:09] But there are specific experiences that sort of indicated to you that there would be essentially an audience for this. Yes. So the one that I like to point to is what happened to Dr. Scott Kennard.
[00:04:23] I convinced Scott to come on the podcast after literally years to tell his story. But Dr. Kennard, PCP, graduated top of his class. He said he thought he was all that in a bag of chips.
[00:04:36] That's kind of how he describes how he felt when he went into practice. He was doing his PCP thing. He had three patients who came to him who were relatively young and all of them died. And they died within 90 days of seeing him.
[00:04:56] And he was devastated, just devastated. He went back and looked at the chart notes after he had seen these patients and he noticed that they all had risk factors. But what they told him was, Doc, I feel fine. I feel fine.
[00:05:12] And what he realized was is that if you take that at face value, you're treating symptoms as a PCP. And if you really want to afford patients better health the way that he puts it, if
[00:05:24] you want to add years to your life and life to your years by taking ownership of your health, as a PCP, you really have to be a risk manager almost. So he disassembled his whole practice and basically put it back together again.
[00:05:37] He's probably one of the first advanced primary care practices. They started doing in his practice all kinds of things. They did, you know, someone had diabetes. They followed a whole care flow to ensure that that patient's diabetes was taken care of. They did the vaccination schedules.
[00:05:55] They did all kinds of things. They had a whole team that surrounded the doctors through some mergers and acquisitions. They eventually grew to 500 physicians. Wow. Yeah. 500 PCPs. 500 PCPs. So this was a big practice in North Texas.
[00:06:09] It was interesting, actually, the payer reactions to what was going on over there. You had one payer, a regional, who had calculated the total cost of care of Dr. Kinnard's patients, Scott's patients, and the whole, I mean the whole group's patients, and gave them an award
[00:06:29] for saving 17% off the total cost of care. So in the context of driving value, I think it's a pretty clear value win. You would think, except there's two national payers who are about ready to kick him out
[00:06:42] of network because the PCP is, you know, as per benchmark, he was 2% or 3% over benchmark for what a PCP should cost. Because if you have a patient with diabetes and you keep bringing them back to ensure
[00:06:54] that they are following their prescribed therapy, your PCP costs are going to be higher. The preventive cost is higher. The acute cost is lower. Yeah. So despite the fact that if he did the math, he's saving 17% over all. If he didn't do the math, he's more expensive.
[00:07:10] So fast forward, the group decides that maybe it would be a good idea to form an ACO. So they decide that they want to form an ACO with a hospital. There's a big local hospital system that is in the area. It had like 16 hospitals or something.
[00:07:28] So his group approaches that hospital system and says, hey, we should form an ACO together. This is at the very beginning of the whole ACO launch. The hospital says, you know what? Thanks for the pitch. We'll get back to you.
[00:07:40] A couple of days later, they call up and they say, you know what? We'd love to do an ACO with you. Here's the thing though. We were kind of thinking about it and it probably would be easier, lots of paperwork, et cetera,
[00:07:52] if we have two tax ID numbers in this mix. So we should just have one tax ID number. So we think that the best idea here would be if we buy you. So we're going to buy you and then we're going to do the ACO together.
[00:08:05] Seems like a good idea. You'd think. The sale transpires. Scott says he describes what happened within a relatively short period of time as his pelican brief moment. He's sitting all by himself in his office.
[00:08:25] His whole entire team is reassigned or let go, or he's all alone in his office. He goes to the chief strategy officer at the health system and he says, what just happened here? And the chief strategy officer at the hospital says, look, Scott, we looked over, you know,
[00:08:43] when you approached us, we actually looked at your doctors and we realized that your physicians had so many fewer ER admits, so many fewer heads in bed, so many fewer acute events that it was our fiduciary responsibility as a health system to shut you down.
[00:09:03] It was our duty to our community that you had to go. Wow. So the primary care practice was dissolved. The way they're operating was dissolved. Oh, it was totally dissolved. The next year, actually, the health care expenditure in that community was $100 million more.
[00:09:21] So that practice of 500 physicians had reduced health care spend in that North Texas area by $100 million. So bringing it back to why you originally started the podcast, what that tells me is
[00:09:33] really the podcast is about creating a community and a forum for folks that want to drive positive change within the health care industry from within. And it's not just about driving change, but sustaining it, which I think is the important second piece that didn't happen in that story.
[00:09:50] Yes. This is what I take away from these stories and why I continue to do this podcast even after 10 years. You know, I do believe that the show is for mission-driven individuals who are just looking to make sure that they don't get themselves in a similar situation.
[00:10:04] So that's kind of like one goal. Another one, though, is that chief strategy officer working at that health system, he quit within a very short period of time because one of the things I think that he realized
[00:10:21] in the course of that was that his values did not align with what happened there. Right. So like that was a big disconnect for him. So the other, I think, big cohort of listeners of Real Out My Self Value are those who work
[00:10:36] for larger corporations who want to understand exactly how they may be contributing to something or not contributing to something that their organizations are doing because they really want to feel like they're in control of the legacy that they leave behind. So that's, I think, a second group.
[00:10:53] Well, one thing I think is so important about the way you approach it is you do take a very cross-industry approach. So you spend time every week talking with smart people from provider organizations, payer organizations, digital health, pharma, employers, really you name it.
[00:11:09] I think that gives you unique depth of insight into how the component parts of our industry are and maybe aren't working together effectively in order to create value. And so I'd love to lean into that this morning because you've done over 430, by my last count, recorded conversations.
[00:11:28] I know there are many more that weren't recorded. So with our time this morning, I would love to work through what are some of the common threads in terms of where are we falling down as an industry? What are some of the common places you see there?
[00:11:40] What are some of the common areas of tension or maybe potentially negotiation for where we can do a better job driving value? And what does it look like when this goes right? So Stacey, let's start with candid conversation of as you think across your conversations
[00:11:57] with folks across the industry, your work with folks across the industry, what are some of the common ways that we are falling down collectively in terms of creating and delivering value? I loved how Dan put it yesterday that when you optimize within your own sphere, and then
[00:12:13] your sphere encounters somebody else's sphere, you could get yourself in a lot of trouble. Like that's when just the value evaporates from the equation. One big example that I often think about is heart failure.
[00:12:28] So heart failure, this is from CMS, is the most common discharge diagnosis among Medicare beneficiaries and the most common cause of hospital readmissions. It's the most costly condition and accounts for $39 billion a year in health care expenditures. It's not subtle.
[00:12:45] One of the reasons why this is a little bit close to my heart is my grandfather had heart failure and watching a loved one, it's like watching your loved one get waterboarded. I mean, they're just like grounding in their own lung fluid.
[00:12:56] I remember one time I went to the ER with my grandparents. We walk in the front door, get triaged. They want to put my grandpa in one of the exam rooms. My grandma, who was a piece of work, says, no, we will not go in that exam room.
[00:13:13] The TV is on the fritz in that one. She knew the rooms well enough to know that the TV in room 7B wasn't working. They had been in that ER so many times. She's familiar with the pros and cons of the various exam rooms. So he'd get admitted.
[00:13:27] He'd get discharged a couple of days later. He'd get the hospital-acquired dementia. He'd get the muscle wasting that elderly patients get when they go in the hospital. He'd come home. It was kind of this downward depression spiral.
[00:13:39] And it was kind of like, don't let the door hit you in the butt on the way out to the parking lot, old man. Like he'd get no med rec. I don't know if his PCP even knew he'd been there.
[00:13:47] One percent of heart failure patients in this country are on optimal medical therapy. One percent? One percent. If you look across the literature, it's pretty clear what you're supposed to do.
[00:13:59] Maybe three or four years ago, I was at a physician summit and a doctor got up on the stage talking about a heart failure program that he had started in his hospital system and it had had amazing results. They were doing some RPM.
[00:14:14] You know, they had connected scales. It was really cool. I was reminded of this because I was talking to Dr. John Lee, who's an ER doctor recently, and he, like two months ago, went to a similar physician summit and another doctor, completely
[00:14:30] unrelated to this first one, got up on the stage and talked about a heart failure, non, you know, reduced readmission program that they had set up. So similar story. Amazing results. Both of us approached the speaker after the presentation and said, wow, that's so amazing. How is it?
[00:14:49] You know, have you expanded the program? How's it going? And both of those speakers sheepishly said, ugh, the second it was over, we got shut down. Pilot didn't move beyond pilot. We you know, or maybe it did for a little bit and then it was ended.
[00:15:08] So what does that tell you in terms of the ways that value was inhibited? So here's a perfect example. Thank you for asking that question. So here's a perfect example of it's unimpeachable patient value from any angle that you look at it.
[00:15:23] This is good for presenting that ED visit so that your grandmother no longer knows which TV in which room is broken. I mean, you think about it from the patient perspective. You think about it from the ultimate purchaser perspective, i.e. taxpayers, self-insured
[00:15:36] employers and other plan sponsors and patients themselves from a financial standpoint for them. This is unimpeachable value. But if you look at it from the hospital system value at the executive level, obviously there was a choice to shut this down.
[00:15:52] But if you look at it from the payer perspective, whoever was involved in that, you know, generally speaking, there's actions and reactions. Right. So you think about why did that program shut down? I don't probably have to do the math for anybody in this room, so I won't.
[00:16:07] But that's the net net of a program that has value for patients unimpeachably and value for the ultimate purchasers unimpeachably. But it still gets shut down. So the spheres colliding. Yeah, the way that I have heard it put so many times is that health care is the only
[00:16:25] industry or one of the few industries where one person orders the dinner, someone else eats it and someone else pays the bill. I love that. That's such a easy to imagine representation of the health care industry.
[00:16:39] Two other points of weakness that I heard in the story that you were telling. One was the fragmentation. You said your grandfather would leave the ED and there's no follow up care. And it was see you next time, essentially.
[00:16:51] And then the other piece is the holistic care, which it sounds like the readmissions programs that you were talking about took the holistic approach to creating value for end user patient. But that might not be a status quo. I would say no.
[00:17:07] Stacey, you mentioned you've been doing Wild Health Values since 2014. And I'm curious how this conversation would have looked different back then. How your answer to this question would have evolved over time. So if I can, for a moment, I want to transport us all back to 2014.
[00:17:24] Amazon has just released Alexa. The FDA just approved a new class of drugs to be used to combat and to drive weight loss called GLP-1s. If anyone remembers the launch of Sexenda. And digital health funding in the US more than doubled from the year before, an eye-watering
[00:17:41] $4 billion. Now for anyone who's keeping track at home, Q1 digital health funding this year was $2.7 billion already. GLP-1s are projected to hit, I think, $100 billion by the end of the decade. And our AI has graduated from telling us the weather to offering differential diagnoses
[00:17:59] and acing medical licensing exams. So with that as a backdrop, how has your answer to this question evolved over time? I think one of the things that's becoming increasingly clear is that as health care becomes more financialized, patient affordability is becoming an increasing difficulty.
[00:18:21] Like I don't think in 2014 it was still on the radar a little bit. But right now there was a survey done of commercially insured patients. 48% of them had delayed or foregone care due to fear of cost.
[00:18:37] Historically we think of that as being more prevalent among the uninsured or underinsured population. But these are commercially insured patients who are functionally uninsured. They have insurance, but they can't afford to use it.
[00:18:48] I mean if you have $400 in your bank account and your deductible is more than that, you can't afford to use your insurance. You can't pay up to the level of your deductible. You have people making clinical decisions for themselves based on financial, you know,
[00:19:07] I've said a million times on the podcast so I sort of stopped saying it. Financial toxicity is clinical toxicity. Which I see more and more when we think about social determinants of health. I see financial health as an increasingly large or an increasingly common factor that
[00:19:24] physicians, clinicians, social workers, really anybody on the care team is looking at. So that certainly resonates. Yeah, I mean you 41, it was KFF the other day, 41% of Americans have medical debt. You know it's just like, oh what's this spot on my arm? Is it melanoma?
[00:19:38] I don't know but it's going to cost me $600 to find out so I'm just gonna see I guess. You're starting to get at almost some cultural realities that we have created.
[00:19:49] One of the things that I love that you talk about on your podcast is this idea of cultural norms that we've created for ourselves within the healthcare industry specifically and how they can actually actively inhibit us from driving value.
[00:20:02] One that stands out to me is the NMP problem. Can you talk a little bit about that? The not my problem problem? I mean you think about that table. You've got the order at the table, right? So call that the provider organization.
[00:20:17] You've got the payer at the table. Call that the carrier. You've got, I mean at this juncture the patient really is sitting at the table deciding what they're going to do or what they're not going to do.
[00:20:27] You have the wallet at the table which again is call it plan sponsor self-insured employers. So it's really easy for things to fall through the cracks if we can go at it this way. Value is always in the eye of the beholder.
[00:20:40] There is a space between you know if I have a capability or as product or service all I have is a capability, a product or a service. It is meaningless until somebody else ascribes it value like the sorcery happens when my
[00:20:55] capability hits the magic of somebody else who thinks it's valuable. So I think sometimes we forget that whatever we're doing over here has to make it the whole way around that table such that value can be realized and if everyone around the table
[00:21:11] is like not my problem and the orderer doesn't see not the orderer's problem to order it, it's not the payers, you know they're like no I don't really see how this benefits me. To me it's an issue of accountability essentially and if nobody's in the driver's seat then
[00:21:28] how do you drive accountability for the patient outcome essentially and what you're saying is that the patient who's in the driver's seat they aren't the ones that you know their feet can't reach the pedals and they don't have the key to the ignition which is a suboptimal
[00:21:41] way to operate. Totally but you know you also think about it healthcare is local. It's also very intimate and it's between it's a relationship between a doctor and the patient and if that relationship isn't there, if there's not trust and a relationship between the patient
[00:21:56] and the satellite he brought up first then nothing's gonna happen ultimately like the patient is not gonna walk out and say I don't really trust my doctor. He told me to take this but you know I don't trust big insert something here right so I'm
[00:22:09] not gonna do it right if you don't have that trust. So you've got healthcare is local but a lot of organizations are national. So it's also not just a not my problem problem and also could be it's not a big enough problem
[00:22:22] for me to worry about problem or it's a I can't figure out how to scale that problem so you know I can't figure out how to solve that problem in all these local markets nationally so we can't really do it.
[00:22:35] So there's a lot of different ways that a problem can become a not my problem problem or it's not a big enough problem or a national problem. So there's I guess a whole bunch of flavors of that.
[00:22:47] It's not always clear to whom you are accountable for driving value. Are we prioritizing driving value for a single patient or driving value for a population and there's not one right or wrong answer to that question but in the examples that
[00:23:00] you're sharing Stacey I'm hearing more value for one stakeholder might be diametrically opposed to value for another stakeholder or not even diametrically opposed but maybe not 100% aligned. Totally and the one thing that I would also say is that a lot of times we talk about those
[00:23:18] stakeholders like a homogeneous blob you know what I mean like payer and it's everybody or hospital system everybody but not only is there variation between hospital systems and payers and you know just amongst the entities that comprise that grouping but also I mean here's another example.
[00:23:38] You remember the Scott Kennard story that I started with. Here's another doctor Dr. Mike Tuggy in Washington and he had had a similar PCP practice. In his case his practice was owned by the hospital and he was doing very similar things to Dr. Scott Kennard.
[00:23:57] In fact they hadn't realized that his practice was saving $100 PM PM for diabetes patients. PM PM per member per month? Per member per month yeah and it was going gangbusters for a number of years.
[00:24:09] One executive changed the executive at the hospital who is I guess overseeing the ambulatory stuff and the new guy shut it down. We're talking about these health systems also like they kind of move lockstep but they don't right like it's only the Democratic votes get taken.
[00:24:26] Should we do this? All say aye. Which can also on the flip side be a very motivating statement. It takes convincing one individual and then that individual can convince other individuals. So let's talk about going over to our website and typing your email address in the box to
[00:24:44] get the weekly email about the show that has come out. Sometimes people don't do that because they have subscribed on iTunes or Spotify and or we're friends on LinkedIn. What you get in that email is a full and unredacted unedited version of the whole introduction
[00:25:03] of the show transcribed. There's also show notes with timestamps so you get everything that you need to decide if you want to list it or not. Just apprising you of the options that are available.
[00:25:14] I want to talk about what are some of the bargaining chips and do a positive reframe of the four tensions because I think it's I think it's accurate. What are some of the bargaining chips that stakeholders in their in all their forms of
[00:25:27] diversity have available to them to try and align more closely on value? You could consider those four bars tensions where we looked at value to who value on what timeline what is it output or outcome and then the last one was proven experimental.
[00:25:45] You could also look at them I think as continuums because it's interesting that you think about the when timeline is it short term or is it long term? There's kind of this implicit assumption a lot of times that those two things are at counterpoint.
[00:25:58] If we achieve short term gains then that is at the expense of long term something and might be true. It is true sometimes but it doesn't have to be true. In other words there's not necessarily a tradeoff, a zero sum tradeoff.
[00:26:15] Yeah you think about okay let's just think about short term. You could also here's some other words for short term minimum viable product. That's the whole point of doing something short term is to create a minimum viable product
[00:26:27] so that you can suss out what's going to work in your quest to build it out further and then achieve long term value. So I would say that one of the biggest ways to try to figure out how to bargain for value
[00:26:45] is to try to figure out if you are working with someone who needs short term wins how to make that short term win actually be the first step toward a long term win which gets
[00:26:57] you closer to all of the things that were on the right side of that like working for outcomes and not outputs etc. So almost the timeline as the stepping stone to drive value in different ways.
[00:27:09] Yeah if you're sitting around a table trying to collaborate everybody around that table has to you know like you think about the orderer in our business the orderer also gets paid. So like everybody around that table they have some self-interest in that equation. Let's use an example. Okay.
[00:27:29] SureScripts is an example of competitors getting together creating a value alliance. Right. I mean the PBMs are the ones that stood up SureScripts which is the electronic prescribing pipes. Like why did they do that? These are fierce competitors who worked together to stand up e-prescribing.
[00:27:52] There's a book it's called Finding Allies. It was written by Mike Leavitt who was the former governor of Utah. It's an interesting book actually. And one of the things that he said is that in order for entities to work together at
[00:28:04] the corporate level there has to be a common pain that's bigger than anybody's kind of day to day I'm going to fight you. Which is almost the flip side of we need to find finding common value start with a common pain or common detractor of value. Yes.
[00:28:22] And then when we're thinking about okay what are these bargaining chips that we can use? We talked about timeline short I don't want to say short term versus long term. Short term on a spectrum to long term. What about metrics?
[00:28:36] If you and I are trying to negotiate work together and we represent different stakeholder entities what are the things that we can try and align on? You can only measure value four ways. Clinically identified outcomes. So clinician identified outcomes like a clinician says that's an outcome patient.
[00:28:56] PROMs patient reported outcomes. Then you have financial outcome and then some kind of performance outcome. Like for example some are better than others. Patient engagement patient satisfaction number of prescriptions written that was the one cerebral used. Right. So like process metric. Some kind of process metric. Right.
[00:29:15] So those are the four ways that you can measure value. If you're thinking about how do you collaborate with a different stakeholder what you have to be thinking about is what do they want to do? Back to your idea of values in the eye of the beholder. Yeah.
[00:29:28] So a huge success story is Rosen Hotels in Florida which gets talked about a lot in employer circles but maybe not so much here. Rosen Hotels they have a big workforce of hotel workers rates are lower paid expensive population typically high turnover.
[00:29:48] They worked together with local providers for the most part and did a number of different things in conjunction with local providers. They saved like one hundred million dollars a year their turnover reduced.
[00:30:00] They saved so much money that they now have a college fund not just for their employees but for their local community. Wow. So how did they align? Right. You had the employer who was looking to you know legit increase value benefit over cost.
[00:30:18] And they're defining value in terms of? In terms of employee productivity in terms of lower turnover in terms of presenteeism and absenteeism. Which I think is important to mention because it might not be top of mind for the provider
[00:30:32] organization who may or may not measure value in terms of employee absenteeism. Exactly but you had enough provider organizations with amazing dedicated clinicians who also wanted to look at what is health. It's making sure that you can show up at work and you can do your job.
[00:30:51] So they worked with provider organizations and they pay them in capitated ways. So you know it's kind of a great thing if you tell a primary care doctor oh by the way you're not going to have to put all those little codes in the computer anymore.
[00:31:02] You know your job is to keep my members healthy. You have Morgan House right now investing in primary care. Lots going on in Ohio along those those same lines because there is actually a lot of alignment
[00:31:15] between employers and in particular primary care at this juncture but they're looking to expand into specialty into pharmacy actually to do total cost of care stuff. I am actually I want to stick with this employer lens for a minute because I'm particularly
[00:31:30] interested in how employers are thinking about the fourth tension which is this idea of proven versus experimental treatments. I think this is a tension that's going to be more important in the next five years than
[00:31:42] it was in the past five years when we think about the pace of innovation and the pace of change. I mean the FDA approved more new therapeutic treatments in 2023 compared to the average of the previous decade. It was 71 last year compared to 53 for the past decade.
[00:32:01] That's a lot and when we look at the graph that we had up yesterday there were a lot of payers that said we measure value or we on the spectrum of proven to experimental. We like 10 years of evidence.
[00:32:14] That means that 71 therapeutics might not be showing up as covered benefits for a decade and that number is only going to increase. So I'm curious about the employer angle or lens on this idea of proven versus experimental.
[00:32:29] Employers I have never I think every single day I get invited to four webinars on what are we going to do with GLP ones and what are we going to do with Selengine literally every day. Yeah I'm not surprised.
[00:32:43] You know if you think about a self-insured employer they're the ultimate purchaser so it's coming out of their pocket. You can have one patient that costs as much as everybody else combined.
[00:32:56] Well and just like we talk about not all of any stakeholder group it's not a modulus group so you've got large employers that might be able to do some risk pooling and you've got really small employers that absolutely couldn't. And what does that mean for patient access?
[00:33:10] Exactly and so I'm hearing there's a lot of creativity actually going on right now because this is it's existential for even some jumbos. They're talking about having generally speaking pharma drugs are tiered so you'll have the proven tiers and then another one that's called the experimental tier.
[00:33:30] And effectively they're basically saying look member if you recognize that this drug is experimental it may or may not work and if you want it then you are going to have to pay more for it.
[00:33:42] And if you want to take that risk then we'll contribute also but we're not going to contribute as much as if the drug is proven. So I'm hearing that bandied about I'm hearing employers trying to get together directly
[00:33:56] talk about collaboration and doing some risk pooling there's some stuff with stop loss right like it's just we're in this weird spot where you know you talk about time being short term long term. That's a huge issue for employers because if you have a cost effectiveness study that's
[00:34:13] being done over a lifetime. You probably don't have it in play for their entire lifetime. Most of the time that's not the case so there's just this kind of time disconnect that's happening right now which is causing a lot of friction right now.
[00:34:26] Yeah I also say I mean we talk about employer lens and I don't mean to position it as though everybody in this room is also not from an employer organization because we are. I think I think something that is important as folks are going through that conversation
[00:34:39] is having a concept of what is value to our organization. I know this is something that you're particularly passionate about is having your stake in the ground around how do I define value for myself for my work to guide my decision making.
[00:34:54] You've actually created a manifesto or a charter of what is value to me. We share that with us. Absolutely and manifesto makes great radio. I would basically say it's more of a statement of values.
[00:35:09] It's what are my values so that I can ensure that at the end of the day the actions that I take are aligned with my feelings of what is personal integrity here. So here's my manifesto.
[00:35:20] The first part is everything that I do will be a net positive for patients. For patients. Yeah. Net positive for patients. The second and third parts are kind of clarifications I think of the first.
[00:35:32] One of them is that I personally tend to focus on short term to medium term timeline. And then the third bit is that it will take a village and that can kind of take two parts.
[00:35:45] One of the parts is who do I need to work with to ensure that it is actually a net positive. But then the other piece of that is who do I need to make sure is doing something else to make sure. Same one. Think about it this way.
[00:35:57] You've got incremental change and you've got disruptive change. And a lot of times those two things are put on counterpoint right. I was reading this LinkedIn exchange the other day and somebody wrote, This is my goal.
[00:36:11] I think I'm going to dedicate my life to ensuring that patients get better value for the dollar of health care that gets spent. Something like that. I read it and I'm like, I don't know. Like. Sure. Literally 30 seconds later someone responds, That's a toxic way of thinking.
[00:36:32] If you're not putting patients in cash pay models, you're part of the problem. So therein is the tension between incremental thinking. So the first guy was like, you know, I'm going to work within the existing system and I want
[00:36:50] to make sure that, you know, grandpa doesn't get readmitted. This one was like, you know what? It's that Buckminster Fuller quote. If you're going to change a system, you can't work within the existing system. You got to rip it down and start again. Right.
[00:37:05] So this guy was in this school of thought. So a lot of the things that we do, we're doing, you know, we just talked about you got to satisfy all the self-interest parties around the table.
[00:37:15] Like a lot of the stuff that we do is we're creating programs that actually worked in the real world and for them to work in the real world, you've got to satisfy, you know, is it optimal if you think about it like let's start from scratch?
[00:37:27] We got to do this and then we got to pay our rebate and blah, blah, blah. So like if you think about it in the actual world, you have to do these things because you're not going to get any value realized if your 500 physician practice gets shut down.
[00:37:42] On the other side, again, if you had to start again, you would not do those things. So I guess the way that I think about it is I am more in the incremental world.
[00:37:53] I'm going to do incremental things, but I kind of want to be keeping my eye out and making sure that there's entities that are working on disruptive things also. Which to me actually goes back a little bit to the proven versus experimental.
[00:38:07] The proven, if we use almost an analogy of the proven is the system that we have and the experimental or the innovation is what's coming in. It's let's work within what we know while being able to adapt and adopt what might be
[00:38:21] coming or what we hope is coming. One thing that I think is important to underscore and why I so appreciate that you have a value statement that you have written down is because we actually all, whether intentionally or inadvertently,
[00:38:34] we create definitions of value for ourselves in our work, in the work that we do every day and then we either recreate it or reinforce it. And I think hearing that from you pushed me to think about am I exercising the definition
[00:38:48] of value that I want to be for the customers that I serve, for the organization that I'm within. So I very much appreciate that. Stacey, as we close down our time, what parting advice would you give to folks from across
[00:39:00] the industry that we have here about how they can take what they learned this week and go forth and drive value in their roles? The one thing that I would say is everybody in this room, I'm assuming that you come to
[00:39:12] a value summit because you are very interested in trying to do the right thing. And that can be hard and it can be dispiriting and you take three steps forward and five steps back.
[00:39:24] So the one thing that I always say is really be kind to yourself and not strive for perfect. If you look back and you see that six months ago, it's better than it was before, then really take a lot of pride in that.
[00:39:41] Great progress is what I'm hearing. So great progress, please. Hey, could I ask you to do me a favor? If you are part of the relentless tribe working hard to transform healthcare in this country,
[00:39:53] I don't need to tell you that we need as many on our side as we can get. The most vital thing that you could do to help expand the reach of this show is to leave
[00:40:02] a rating or a review on iTunes or Spotify and or share this show with colleagues or decision makers. I cannot appreciate it more when I see the reviews and they really count towards our search rankings. Thanks so much for listening.